Following are links surrounding the debate as to whether to aspirate the syringe before injecting a vaccine, especially the COVID-19 vaccines, to ensure the liquid is injected into the muscle tissue and not a vein. If blood is drawn back into the syringe, by “aspirating the needle”, it indicates you’ve struck a vein, thus the injection would be intravenous (at least in part), and not intramuscular.
“An injection is defined by the World Health Organization (WHO) as parenteral administration of medication through a skin puncture via a syringe, while aspiration is defined as the pulling back of the plunger of a syringe (for 5–10 seconds) prior to injecting medicine. Aspiration is most commonly performed during an intramuscular [IM] or subcutaneous [SC] injection, and is meant to ensure that the needle tip is located at the desired site, and has not accidentally punctured a blood vessel.” [1]
Muscle tissue has a generous blood supply (but according to the WHO no large veins so not relevant), Flu and COVID-19 injections are said to be delivered intramuscular, but given this terrain, how can one be certain of the target (tissue or vein) without aspirating?
- Could failing to aspirating lead to more adverse events through inadvertent venous injection?
- Did the clinical trial participants have their injections aspirated?
CDC’s position on aspiration
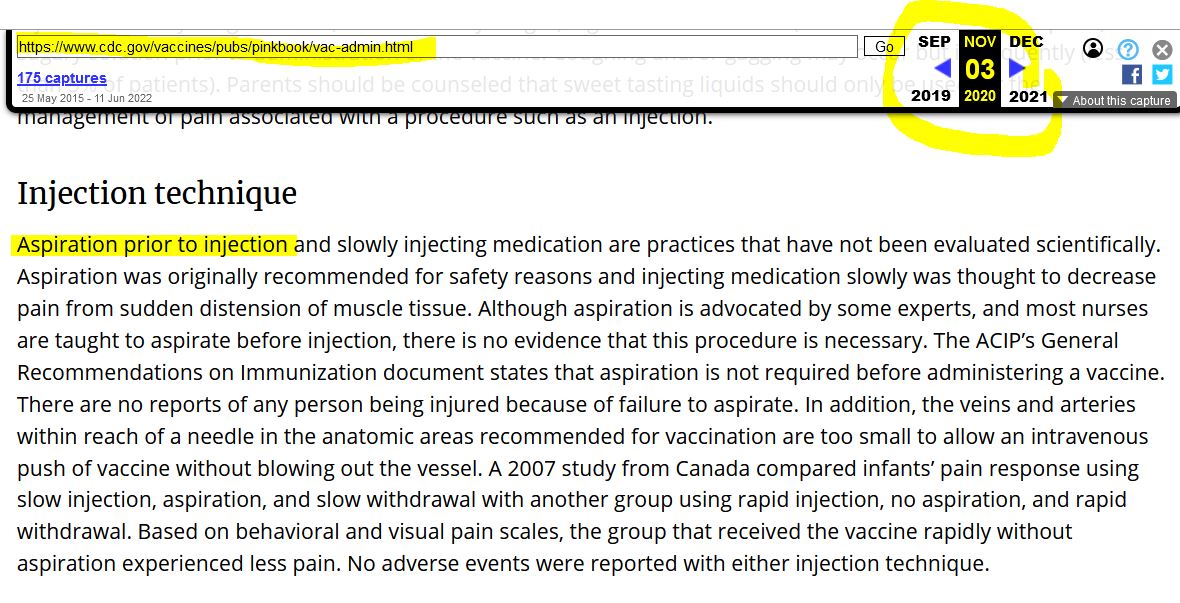
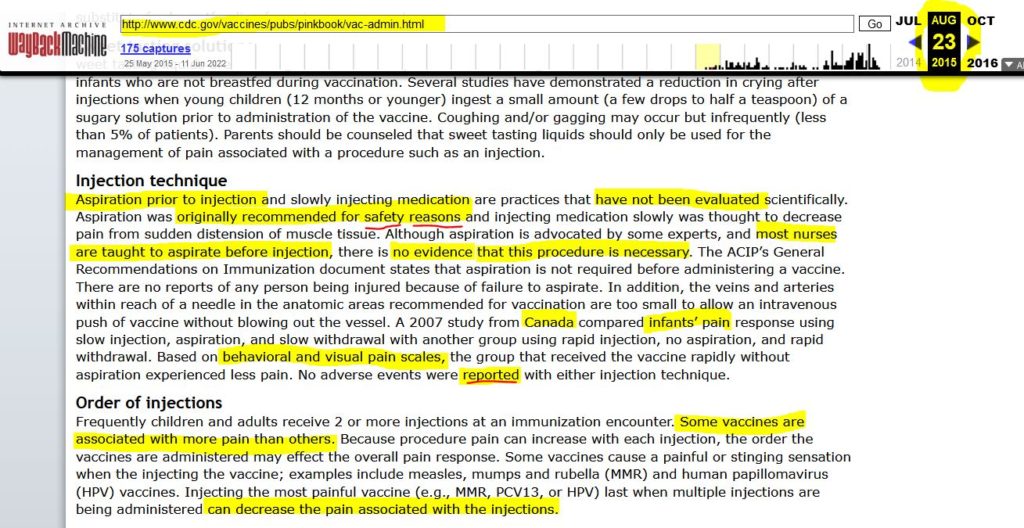
The CDC’s reason for not aspirating the syringe before administering any vaccine is because the procedure can increase pain. – ARCHIVE
The CDC Pink Book vaccine administration guidelines – HERE
What exactly is the risk of hitting or severing a vein in the process of administering a vaccine?
Could the nano-particles enter a small vessel if it is severed, even if the bulk of the “vaccine” is administered into the deltoid muscle?
Could the Bolus Effect account for the post injection adverse events?
- The Bolus Effect “The Needle’s Secret” by Marc Girardot – SUBSTACK
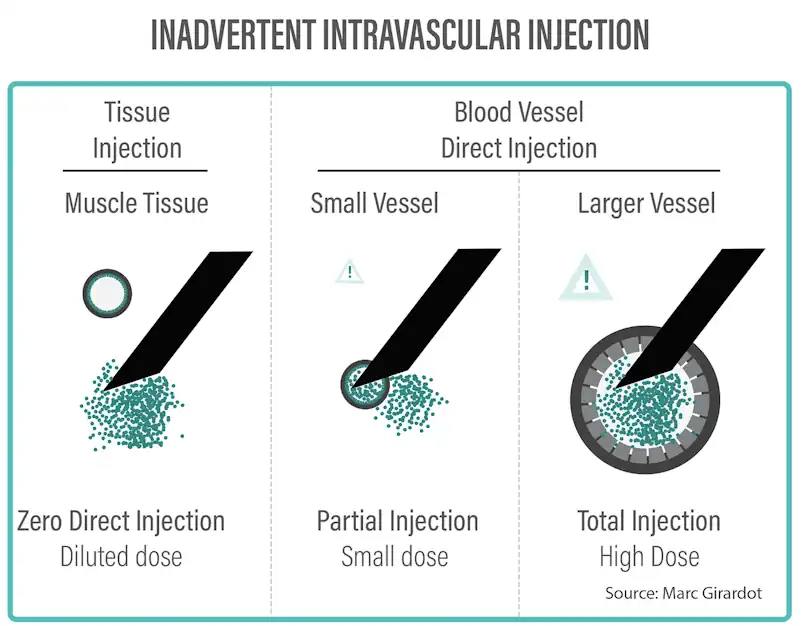
Inadvertent Intravascular injection scenarios – source
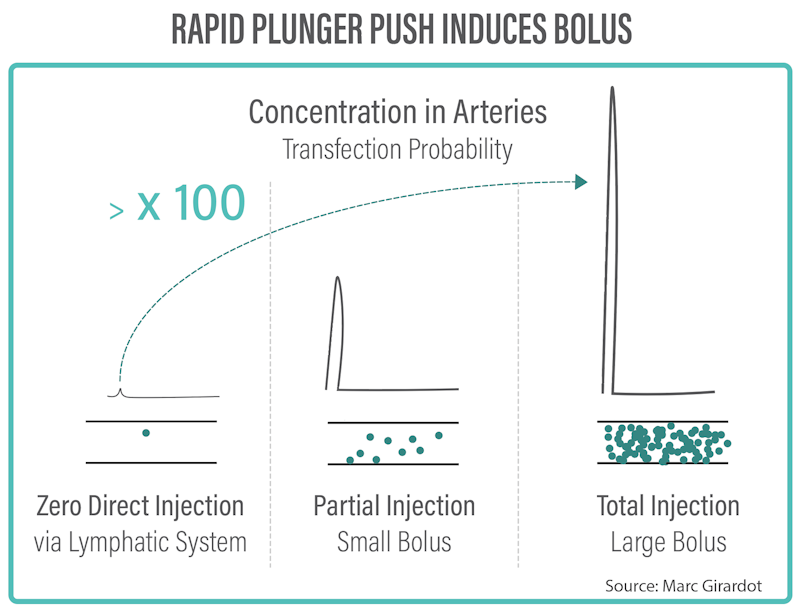
Rapid plunger push induces bolus scenarios – source
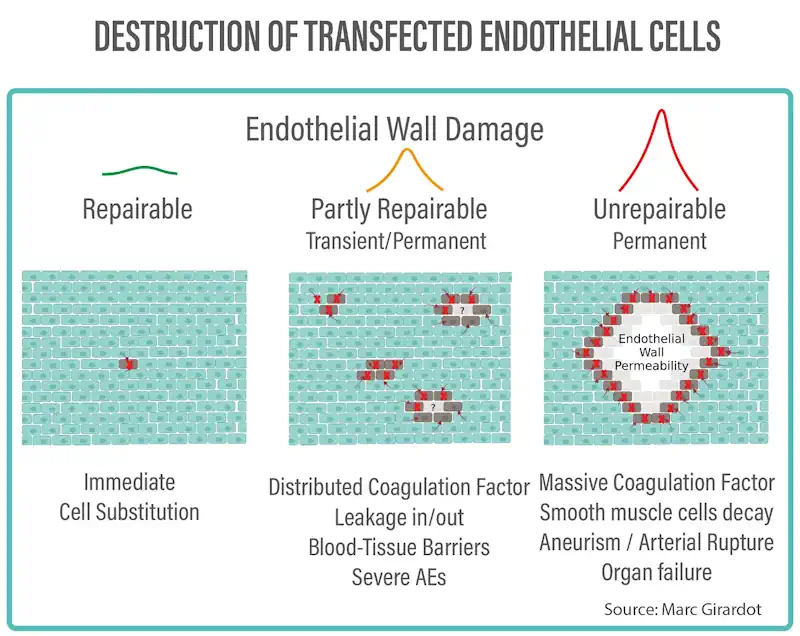
Destruction of transfected endothelial cells scenarios – source
CDC – Prevaccination Screening Checklist for COVID-19 Vaccines (no mention of aspiration)
Articles and information in reverse chronological order
2023
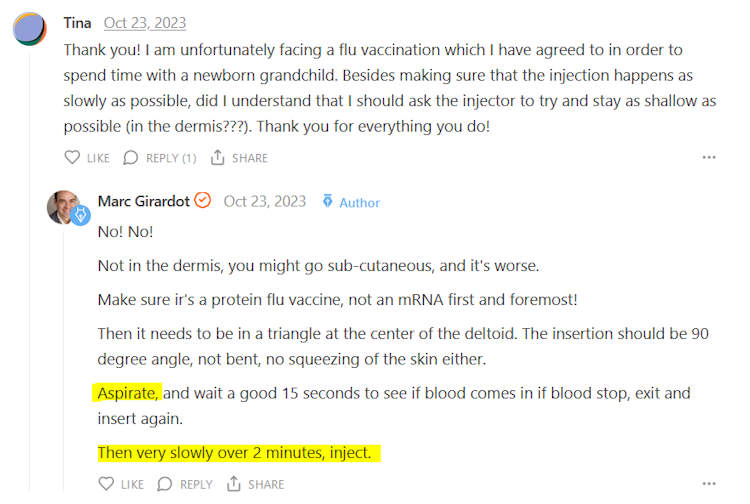
October 22, 2023 – Covid Myth Buster Series by Marc Girardot: The Bolus Theory – Upcoming book “The Needle’s Secret” is nearly finished. The Bolus Theory today is the only reproducible theory, validated on animals, explaining all the vaccine adverse events and spanning all vaccines – READ, CREDIT
- Accidental intraveneious injection followed by a bolus of syringe contents is the Bolus Theory of harm
- “I went on to check forty different ways the injection could harm from specific endocrine disorders to cancer, from Parkinson’s disease to heart defects, from Guillain-Barré to blindness…” all 40 came true
- “My friend, a Nobel Prize winner as well as a Professor of BioPhysics, exclaimed a loud: “Wow!”.”
- “As a society, we have been harming ourselves with billions of inadvertent IV injections for over a century, a form of industrial accident, a massive invisible off-protocol mishap that we are blindly accelerating upon in a form of societal suicide.”
- “Based on steroid injections WITH ASPIRATION and by trained nurses, 2% go IV….So without aspiration and with untrained, most likely 5% go IV…Not pulling blood doesn’t mean you are not injecting in IV…” MG from comments
February 24, 2023 – Dr John Campbell: Aspiration – Why is this not being done, it is in Denmark – WATCH
2022
October 3, 2022 – Rebel News: COVID-19: Dr. Byram Bridle discusses mRNA in breast milk and how the study leaves him with more questions than answers – WATCH
- We were all told the injection mRNA stays in the shoulder muscle,… The recent paper shows “babies are consuming the vaccine” that their mother was given. Oral administration has never been tested!!!!
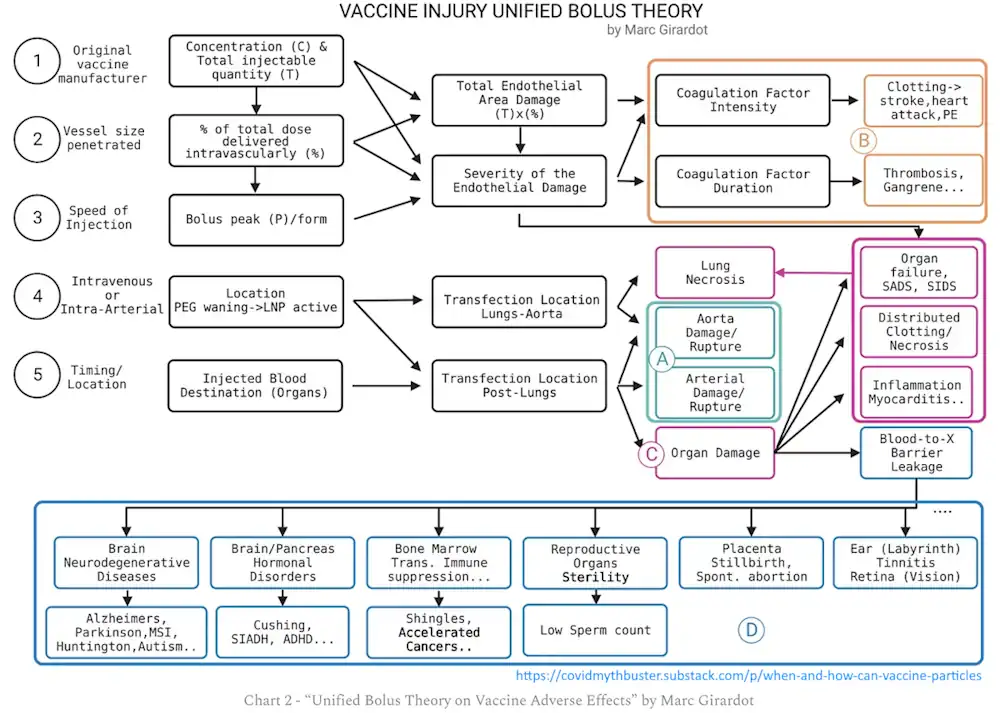
September 12, 2022 – Marc Girardot Substack: When and How Can Vaccine Particles Hurt You? – A Visualisation Exercise – The Bolus Theory – READ
March 23, 2022 – Pharmacological Reports: To aspirate or not to aspirate? Considerations for the COVID-19 vaccines – READ
- “Syringe aspiration when vaccinating intramuscularly was not recommended before the pandemic due to the lack of conclusive evidence that it provides any benefit. However, in vivo evidence suggests that intravenous injection of mRNA vaccine can potentially lead to myocardits while introducing adenoviral vector to bloodstream can possibly result in thrombocytopenia and coagulopathy.
- Although the syringe aspiration may increase the level of pain at the injection site, it represents a simple technique to decrease the risk of vaccine introduction into the vascular system and potentially decrease the risk of severe reactions to mRNA and adenoviral vaccines.” …”[A]spiration when giving mRNA and adenoviral vaccines appears to be fully in line with the precautionary principle.”
January 22, 2022 – Elsevier Public Health Emergency Collection: Aspiration before intramuscular vaccines injection, should the debate continue? – READ
- They summarise the broad reasons why the CDC & WHO no longer [since 2015] recommend aspiration, even though it was common:
- the absence of large vessels in the deltoid area (yet 40% nurses aspirate blood!)
- increased pain (assumed vaccine hesitancy, and assumed infant pain is the same as adolescent or adult pain!)
- lack of evidence in favour of the aspiration technique (there is not research!)
- syringes which do not allow aspiration does do not appear to have been associated with increased adverse events in mass campaigns
- The note “intravascular injection of vaccines is formally contraindicated”, meaning injecting into a vein is not a good thing! “The justification for aspiration would be based on the theoretical assumption that it can be seen as a test with the “needle out of the vessel”.
- The aspiration of blood during intramuscular injection in adults does not appear to be rare!
“…there is evidence that intravascular injections of vaccines containing adenoviral vectors are associated in preclinical models with coagulation disturbances, multi-organ failure and death.”
“…the European Medicines Agency has acknowledged a possible link between inadvertent intravascular injection and thrombotic events associated with the AstraZeneca vaccine, although it also admits that this link has not been formally evaluated”
- As they are clear to point out many reviews on aspiration focus on pain and find there are not reports of “adverse effects associated with the aspiration-free technique” but the reviews lack the power to find unusual side effects becasue they:
- do not assess long-term side effects
- do not consider a decrease in vaccine efficacy
- do not include a considerable number of patients
[Let the above sink in. The WHO and CDC have made policy decisions effectively based on reducing vaccine hesitancy policy.]
- These authors conclude that “we must reopen the debate about the appropriateness of aspiration.”
- As the the European Medicines Agency find a potential link to severe thrombosis and the mouse model finds a potential link to myopericarditis.
- Aspiration of the syringe is potentially short term pain for long term gain – in health (should you choose to get vaccinated)!
2021
November 18, 2021 – MSN: No, doctors don’t need to aspirate the injection when giving the COVID-19 vaccine – (in this article they reference WHO and CDC which recommend don’t aspirate because of increased pain, but they cite this mouse study below and justify it’s not relevant to aspiration because they purposely injected into the vein! This is typical media/”doctor” spin) – READ
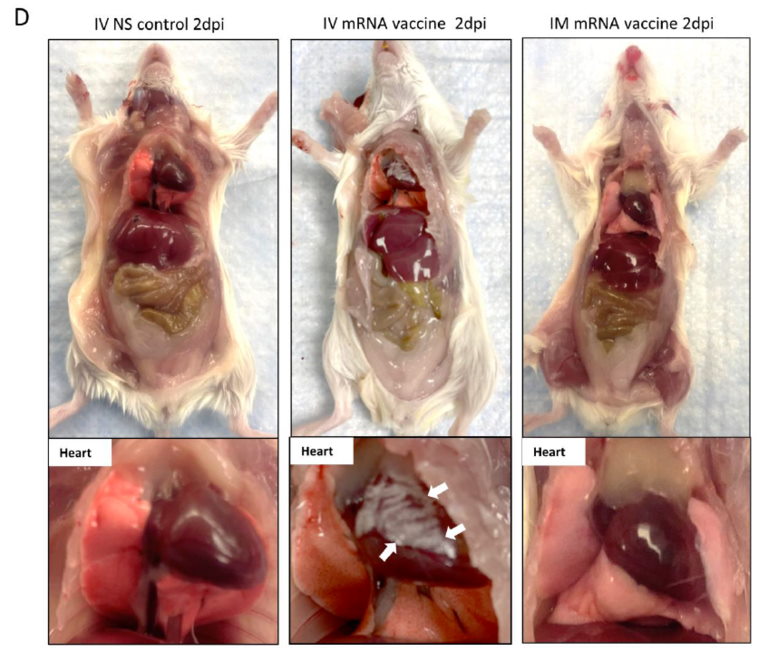
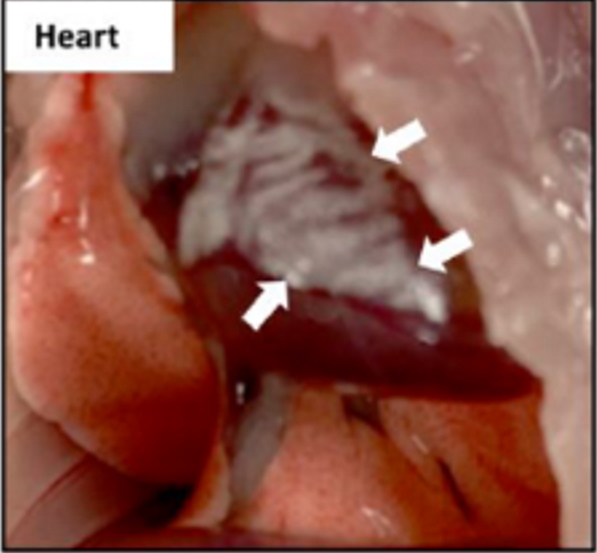
August 18, 2021 – Intravenous Injection of Coronavirus Disease 2019 (COVID-19) mRNA Vaccine Can Induce Acute Myopericarditis in Mouse Model – READ, Naomi Wolf’s response – GETTR, SOURCE
Article amended December 2021 – HERE
Authors conclusion:
Brief withdrawal of syringe plunger to exclude blood aspiration may be one possible way to reduce such risk.
March 1, 2021 – Journal of Nuclear Medicine Technology: Intramuscular Injections for COVID-19 Vaccinations – READ
- “The following protocol specifically addresses the intramuscular administration for the 2 COVID-19 vaccines manufactured by Moderna and Pfizer-BioNTech”
- Stabilize the patient’s arm with the nondominant hand and insert the needle into the injection site at a 90° angle and administer the entire dose. Note: do not aspirate the syringe before or after administering the injection.
January 28, 2021 – Psycology Today: What’s the New Phenomenon Called “COVID Vaccine Arm”? – The eighth day delayed reaction to the Moderna COVID-19 vaccine. – READ
- “With the new mRNA vaccines given to millions of people all around the world, we are in a giant clinical trial and it is our duty to understand and report new vaccine reactions.” [One month since rollout!]
January 9, 2021 – Deccan Hearald: After the Covid-19 vaccine: Sore arm, yes; headache, maybe; regrets, no – READ, also brain fog, tired and achy, “post-vaccine malaise”
- “a nation down for the count with post-vaccine malaise would be the best news in a long time. The side effects dissipate within a few days, and they are a signal, the experts say, that the vaccine is working”
January 8, 2021 – ABC News: Why vaccines are injected in your upper arm muscle, and not in your veins – READ
- Dr Joanna Groom, an immunology researcher at the Walter and Eliza Hall Institute explains the dendritic cell immune response an also says:
- “muscle has an excellent blood supply to help disperse the vaccine”
- “Muscle helps localise any adverse reactions and minimise them, so it’s safer.”
- muscle acts as a “deposit”, where the vaccine can linger a while and be used over a longer period
January 4, 2021 – News Nation Now: Doctor sounds alarm on how to properly inject COVID-19 vaccine – READ
- Dr. Tom Pitts, a board-certified neurologist, says he has been noticing too many injections going out across the United States not being administered the correct way – they need to go into the deltoid muscle
2020
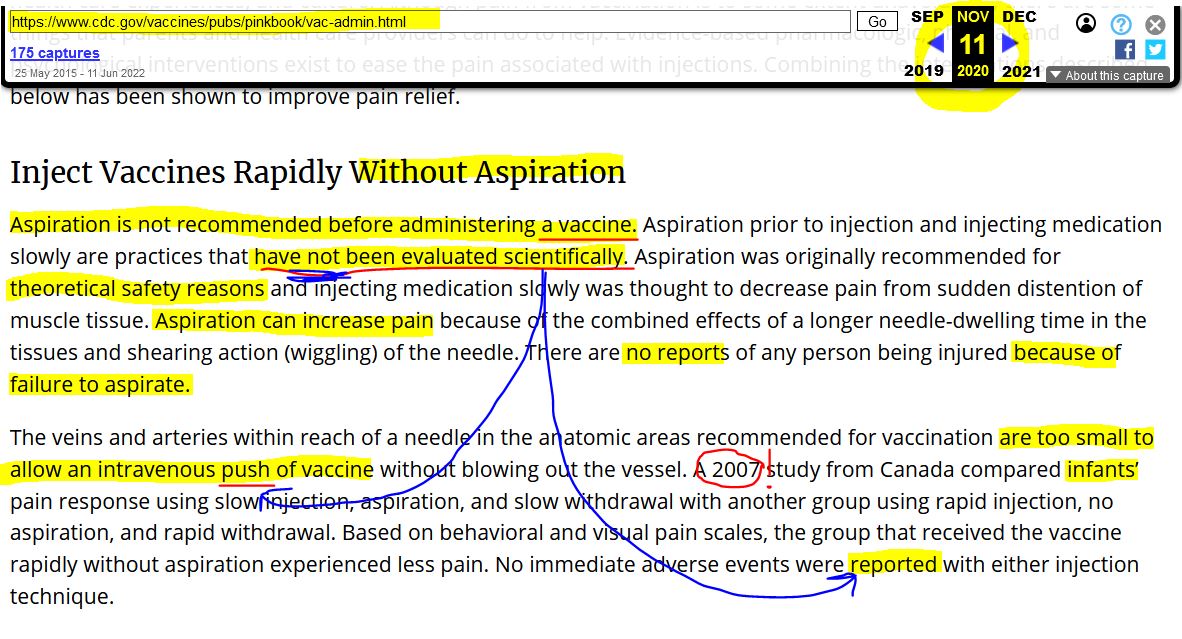
November 11, 2020 – The CDC update their Vaccination Pink book on aspiration, just before the COVID-19 vaccine rollout – ARCHIVE
They admit that aspiration prior to injection has not been evaluated scientifically – so shouldn’t the precautionary principle prevail?
2017
March 1, 2017 – F1000 Research: Aspiration in injections: should we continue or abandon the practice? Version 3 – READ, Sept 4, 2014 – Version 1 – READ (also see below)
“Aspiration during any kind of injection is meant to ensure that the needle tip is at the desired location during this blind procedure.”
“Based on our findings, the need for aspiration prior to administering an injection is dependent upon multiple factors.”
2016
October 25, 2016 – Clinical Nurse Research: Blood Aspiration During IM Injection – READ
A survey of 164 registered nurses who were trained to aspirate, continued to do so even after WHO 2015 policy update. 40% nurses reported having aspirated blood at least once.
2015
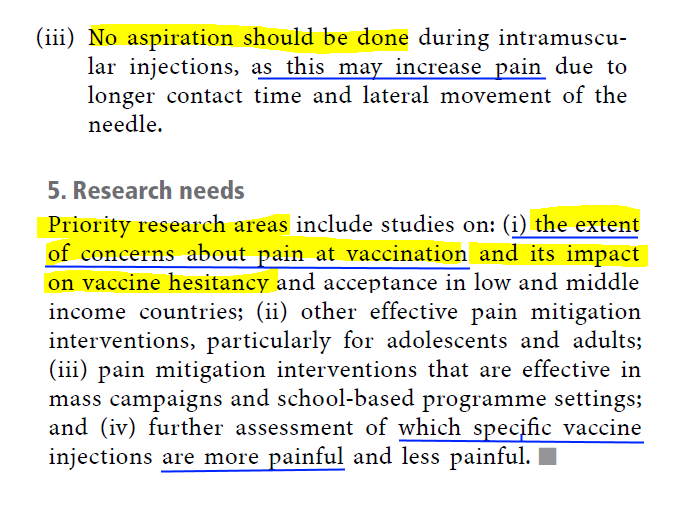
September 25, 2015 – World Health Organisation (WHO) – Weekly epidemiological record 2015 vol. 90, 39 (pp. 505–516) – Reducing pain at the time of vaccination: WHO position paper – READ, WHO, 2015- ARCHIVE
Position Paper process – HERE
Context: “…pain is one of the primary sources of anxiety for caregivers of children receiving multiple injections in one visit”…”Hesitancy towards vaccination can result in lower vaccination coverage rates, putting the individual and the public at risk of vaccine-preventable diseases. A recent [Oct 2014 WHO SAGE] report highlighted pain mitigation at the time of vaccination as an important strategy to counter vaccine hesitancy.”
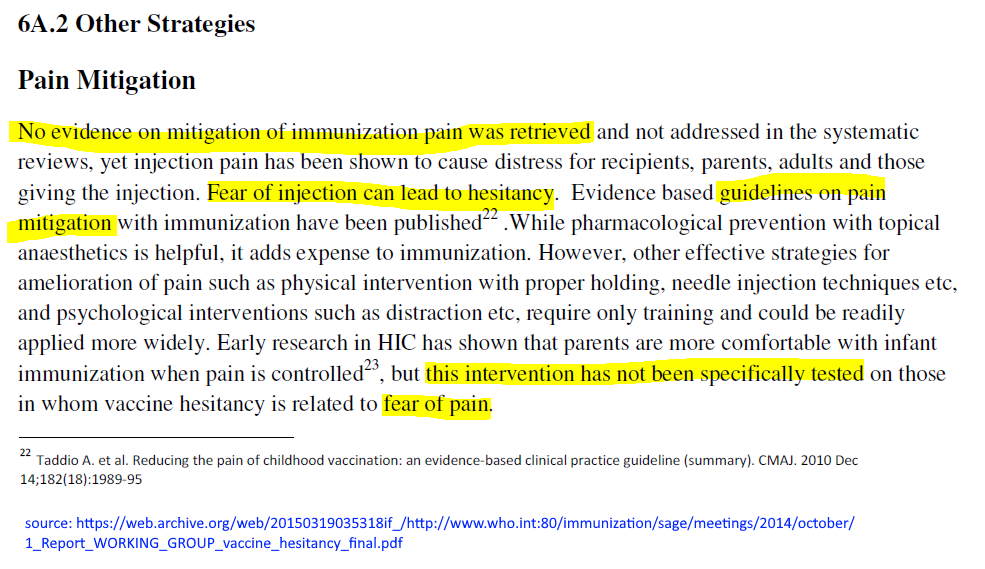
[Actually the 2014 report on vaccine hesitancy, found below, stated the “intervention had not been specifically tested” on those who have “fear of pain.” Just that “Fear of injection can lead to hesitancy”. ]
“This position paper is the first policy paper on pain mitigation at the time of vaccination. It integrates information pertaining to the reduction of pain, distress and fear across all age groups.”
“Pain during vaccination sessions is manageable and managing pain does not decrease the efficacy of the vaccine.” [Does the consequence of managing pain, potentially lead to greater adverse events?]
It appears the WHO’s focus on managing pain is mostly to reduce hesitancy, an assumption (no evidence) that potential pain is a reason for not getting vaccinated. Their policy is to NOT “aspirate the syringe” in order to reduce short-term pain, but they have not evidence to support this is the reason for hesitancy, without considering the potential adverse events that could arise from off-target injection.
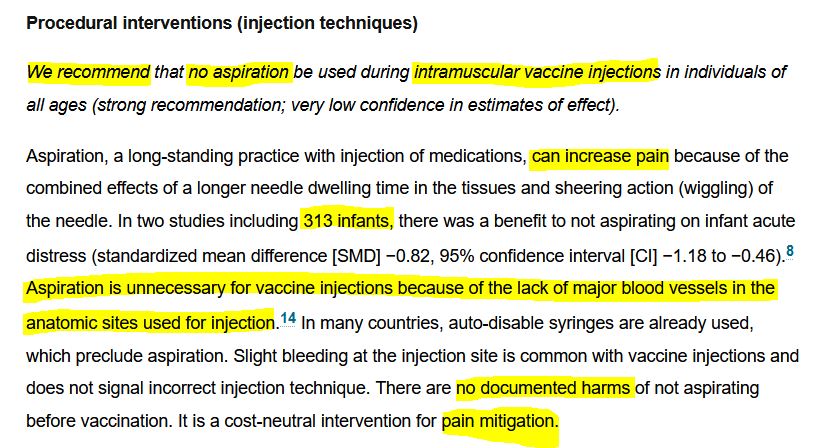
September 22, 2015 – Canadian Medical Association Journal – Reducing pain during vaccine injections: clinical practice guideline (systematic review referenced by WHO above) – READ
- No aspiration because of “lack of major blood vessels”! [Small blood vessels flow into major vessels!]
- “Delayed pain (hours to days after injection) was not considered in this guideline.” [What about adverse reaction due to hitting a vein?]
May 25, 2015 – CDC’s Pink Book guidance on aspiration – same wording May 2015 until 2019 – ARCHIVE
They have not done the safety studies, and rely on a Canadian “pain” study in infants using visual and behavioural cues! Remember, vaccines are said to be “rigorously” tested by FDA & CDC and other global regulators and health agencies.
April 14, 2015 – J. Clin. Nursing: Aspirating during the intramuscular injection procedure: a systematic literature review – READ
“The process of aspiration has been ingrained in the intramuscular injection procedure, and whilst many policies no longer recommend this practice, it often continues to be taught and practiced. The result is a variation in this procedure not always consistent with an evidence-based approach.”
“Owing to its proximity to the gluteal artery, aspiration when using the dorsogluteal site is recommended.”
2014
October 1, 2014 – WHO: REPORT OF THE SAGE WORKING GROUP ON VACCINE HESITANCY – READ
“…vaccine hesitancy is a complex behavioural phenomenon”
“The impact of pain mitigation with immunization on vaccine hesitancy was not included in the systematic review but evidence-based guidelines for addressing pain are available.” pg 40
Sept 4, 2014 – F1000 Research: Aspiration in injections: should we continue or abandon the practice? Version 1 – READ, updated version 2017
- “In this review, we have attempted to gather and present literature on aspiration both from published and non-published sources in order to provide not only an exhaustive review of the subject, but also a starting point for further studies on more specific areas requiring clarification.”
- “In most instances, general clinical or vaccination experiences guide global recommendations for aspiration.” The WHO or CDC or other has not conducted a randomised controlled trial, but then that may also depend on the product being administered and how it could affect the body if receive via a vein.
1980s
1982 – In 1982 genetically modified insulin, so-called ‘human’ insulin, received marketing approval.
1980s – Insulin Injection History – A comment by Susie AH under the Bolus Theory – READ
- “In the 1980s Novonordisk introduced the insulin pen after they developed so called ‘human insulin” by genetically modifying bacteria which then excreted the insulin – that is an interesting story in itself because it was only tested on 25 young healthy non diabetic men before being given to type 1 diabetics. Something called “dead in bed” syndrome then occurred and no-one bothered to connect it to the human insulin, it’s still not acknowledged now but the connection is obvious….Anyway in order to use the pen one was unable to aspirate. They started introducing shorter and shorter needles so the chances of going into anything more than the smallest capillary were small in a subcutaneous injection.”…Prior to the “Novopen” diabetics always aspirated prior to injecting.
- InDependent Diabeties Trust: A Little Bit of History – Genetically Modified vs Animal Insulin – READ
- In 1982 genetically modified insulin, so-called ‘human’ insulin, received marketing approval. Approval was given in five months, a remarkably short time when one realises that it was the first genetically produced drug to be licensed and used on people.”

